
Context: I’m an Australian retired GP with over 20 years of clinical experience in both Family and Emergency Medicine. I’ve had Long Covid for 22 months, of moderate severity, mostly fatigue and PEM with some POTS. At my worst I had to spend 22 hours per day in bed. I’ve gone down many rabbit holes in my search for solutions; my search for solutions has dominated my recent life. I’ve been running a Facebook group dedicated to finding solutions to Long Covid through self experimentation and objective measurements for over a year. I follow every single research lead and am in personal contact with some of the leading doctors and scientists in the space.
I’m relentless in experimenting on myself.
I’ve got an open minded doctor to work with me who respects the knowledge I’ve gained on this disease.
I believe that the #TeamClots work on finding microclots in Long Covid is the biggest breakthrough we have had so far in working out what this disease is and how to treat it.
Those evil and sneaky microclots!
Microclots are different to the big jelly like clots which are well known about in standard medical practice; microclots are little hard nuggety buggers with a consistency more like grains of cooked mince meat. Microclots also behave differently: they are very resistant to breakdown, unlike big jelly clots. The cornerstone of standard medical testing for clots is measuring the breakdown products of clots, the DDimer test. Because microclots hardly break down much and are tiny, microclots are mostly invisible to standard medical diagnosis technology.
As you can imagine, it’s not healthy to have billions of microclots running through your body’s 100,000 kilometers of blood vessels. Microclots are especially good at blocking the smallest blood vessels, the capillaries, so that blood can’t get to all the bits of the body. Every single bodily process relies on having a good blood supply, and the most important thing the blood delivers is oxygen. Just to add insult to injury, platelets are usually overactive in Long Covid as well and add to the blockages of the circulation.
The #TeamClots Professors Resia Pretorius and Douglas Kell have pioneered the use of fluorescent microscopy to see and measure the microclots directly. 100% of people with Long Covid tested so far have them. More on their work is found here: http://dbkgroup.org/longcovid/
An alternative test for microclots: venous blood gas analysis.
Unfortunately, in Australia I can’t access fluorescent microscopy testing: but what I can access in Australia, very easily actually, is peripheral venous blood gas testing from the antecubital fossa (elbow level). As far as I can see, Australians have the easiest access to this test in the world! Your GP can order it easily and it’s Medicare funded. The only restriction is that only certain pathology labs, usually attached to a hospital, do them.
The venous blood gas test is used in standard medical practice in Intensive Care, where the measurement is made via a central line catheter at the top of the heart where the blood comes back after it’s journey through the body, before it’s pumped through the lungs to get re-oxygenated again. It’s normal for it to drop a proportion of it’s oxygen but not usually more than 30% of it, so we always have a reserve.
Long Covid usually has little to do with the lungs. In Long Covid a low venous blood gas oxygen saturation is mostly about what happens in the circulation of the rest of the body.
In most of us with Long Covid there’s more than enough oxygen coming from the heart and lung system. Most of us have experiences of having normal lung Xrays and CT’s, normal heart function, normal pulse oximetry on the finger, among all the other normal tests, so then we are infuriatingly told, “All your tests are normal, it’s all in your head”.
The problem is that a doctor won’t see what’s wrong if they don’t know what to look for. Unfortunately they’re looking in the wrong place. The problem isn’t in the uptake of oxygen from the heart and lungs. The problem is in the delivery of oxygen to the rest of the body.
O2 saturation in venous blood is not generally used in clinical practice outside of Intensive Care, because to measure it properly it needs to be near the heart, and to get there you need to have a really big scary needle shoved into the neck like from a bad science fiction show and plunged deep, deep down to the top of the heart. So the only practical option is to get a sample from the antecubital fossa (the front of the elbow).
Is a blood sample from the antecubital fossa (elbow level) good enough?
This paper I link below shows that peripheral venous oxygen saturation results are quite a bit different to central mixed venous oxygen but they both change in sync with each other. While you might not be able to rely on the absolute value at one test done once, repeated measurements from your elbow level vein will show similar changes to what’s happening centrally. The trend is valid even if the absolute number is not. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6131814/
To maximise the accuracy of this test it’s important to insist on not having a torniquet applied to the arm before the test.
I found out a lot of things from direct communication from patients and doctors involved in apheresis, (blood filtering) especially Dr Asad Khan, a famous respiratory specialist with Long Covid who has had apheresis many times. Very low peripheral venous oxygen saturation is a pretty consistent finding in people with Long Covid and it significantly increases after apheresis. The normal range varies a bit according to different sources, but is usually said to be about 60-80%. Many, if not most people with Long Covid have peripheral venous oxygen saturations of 30-40%. This is reflecting a central venous oxygen saturation which will be even lower.
The Walking Dead.
If we were in Intensive Care, all the doctors would be concerned about these low levels; we would be considered among the sickest patients there. So there’s a huge disconnect with having oxygen delivery problems that are on par with the sickest patients in Intensive Care who are about to die: however we are walking around and look healthy enough (for an hour or two before we crash for a week!). But it finally makes sense: we have to spend most of the day in bed because our bodies ARE really sick. The blood is hardly getting through. We aren’t getting enough oxygen to our brain, muscles and other organs. We have severe, Intensive Care level disease.
My hypothesis was that venous oxygen saturation testing may act as an indirect measure of blockages in the small blood vessels caused by microclotting and platelet activation. Repeated testing could be a way to determine the effectiveness of any treatment directed against microclots. Tracking venous oxygen saturation may give an objective measure of success, or failure.
In the great tradition of Dr Barry Marshall, who tested his ideas by chugging down H Pylori bacteria, I embarked on my self experiment.
My first venous blood gas test result was as below.
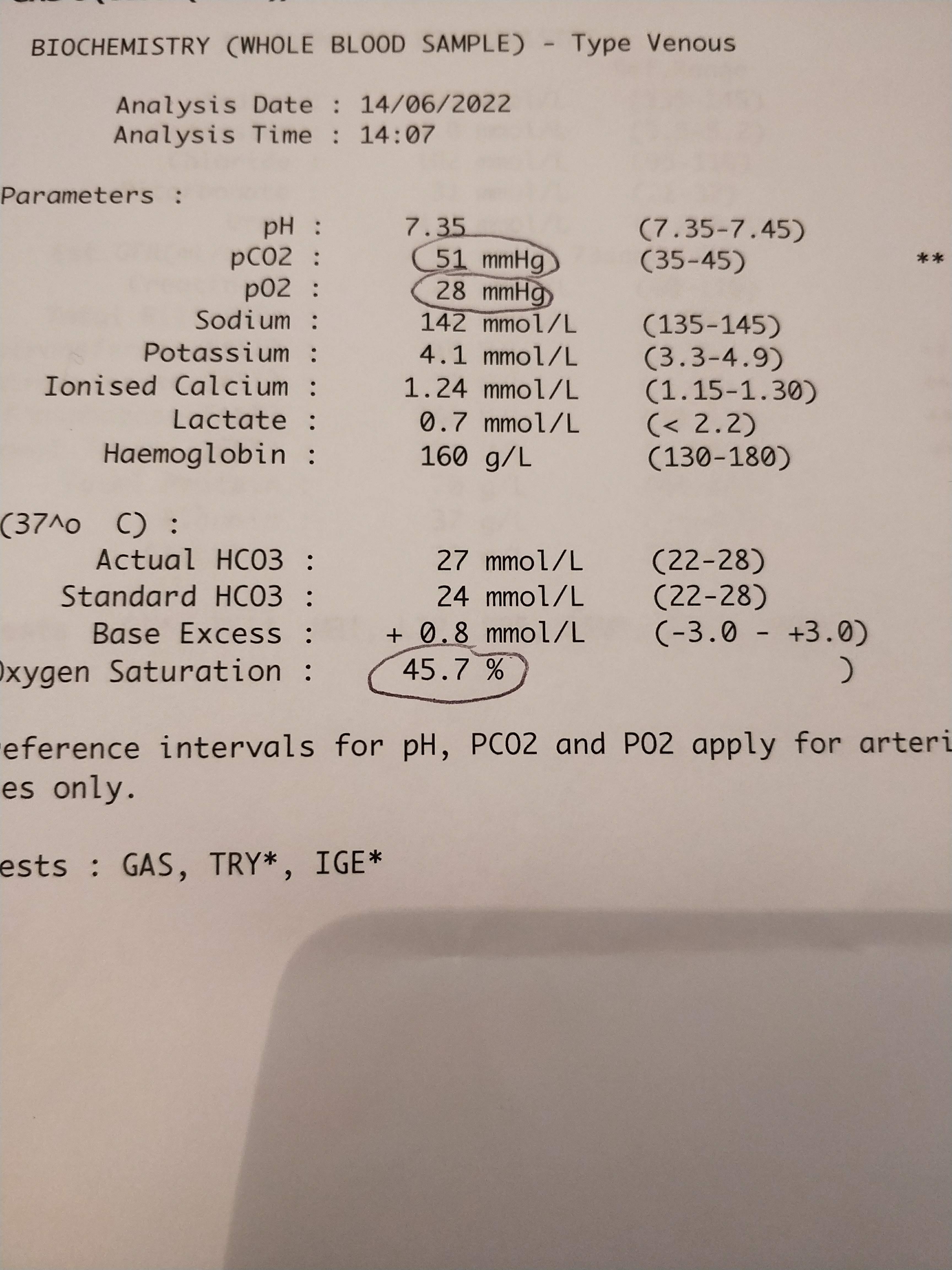
Not as bad as what other people with Long Covid have, but certainly not normal. In the absence of any other pathology I assumed it was microclots and platelet activation. I went on to triple medical anticoagulant treatment; clexane injections, (because it also has action to heal the lining of blood vessels, the glycocalyx) and dual antiplatelet therapy (clopidogrel and aspirin). Many people use oral apixaban instead of the Clexane, and honestly I’m not sure which is better.
Beware: this is dangerous, this is much more powerful blood thinning that what is usually done in medical practice. You have a significant risk of a major bleed to the brain and this should only be done under medical supervision with regular testing of your coagulation and ideally, something called Thromboelastography (TEG) as well.
I thought I may have felt a little better but my venous oxygen saturation refused to budge. I was getting a venous blood gas test every 1-2 weeks.
I was a bit scared by the Clopidogrel after haunting voices in my memories of my surgical rotation being told it was “the devil’s drug” by a surgeon. I had visions of sudden bleeding on the brain. I was willing to take that risk, but not if the numbers refused to budge, and I wasn’t feeling better.
So I dropped the Clopidogrel and added Nattokinase which had worked for me previously at 4000 FU (200 mg) twice a day. It’s also safer, because it doesn’t decrease the ability of the blood to clot as much as it directly dissolves the protein in the microclots. Unfortunately, after a month of this, I was still no better clinically, and still no better in the oxygen saturations.
I really didn’t like the risks I was exposing myself with the Clexane and I really didn’t like injecting myself every day to so I changed tack. I’d heard some anecdotes about a herbal compound called Vedicinals 9 working to clear microclots when triple therapy didn’t. I was sceptical, but desperate. I was in discussion with the manufacturers who strongly warned me against being on any form of anticoagulation whilst on Vedicinals; I might have a serious bleed on the combination. I therefore dropped all the anticoagulants, antiplatelets and Nattokinase and went on Vedicinals alone. But again: no change. In fact, it got worse.
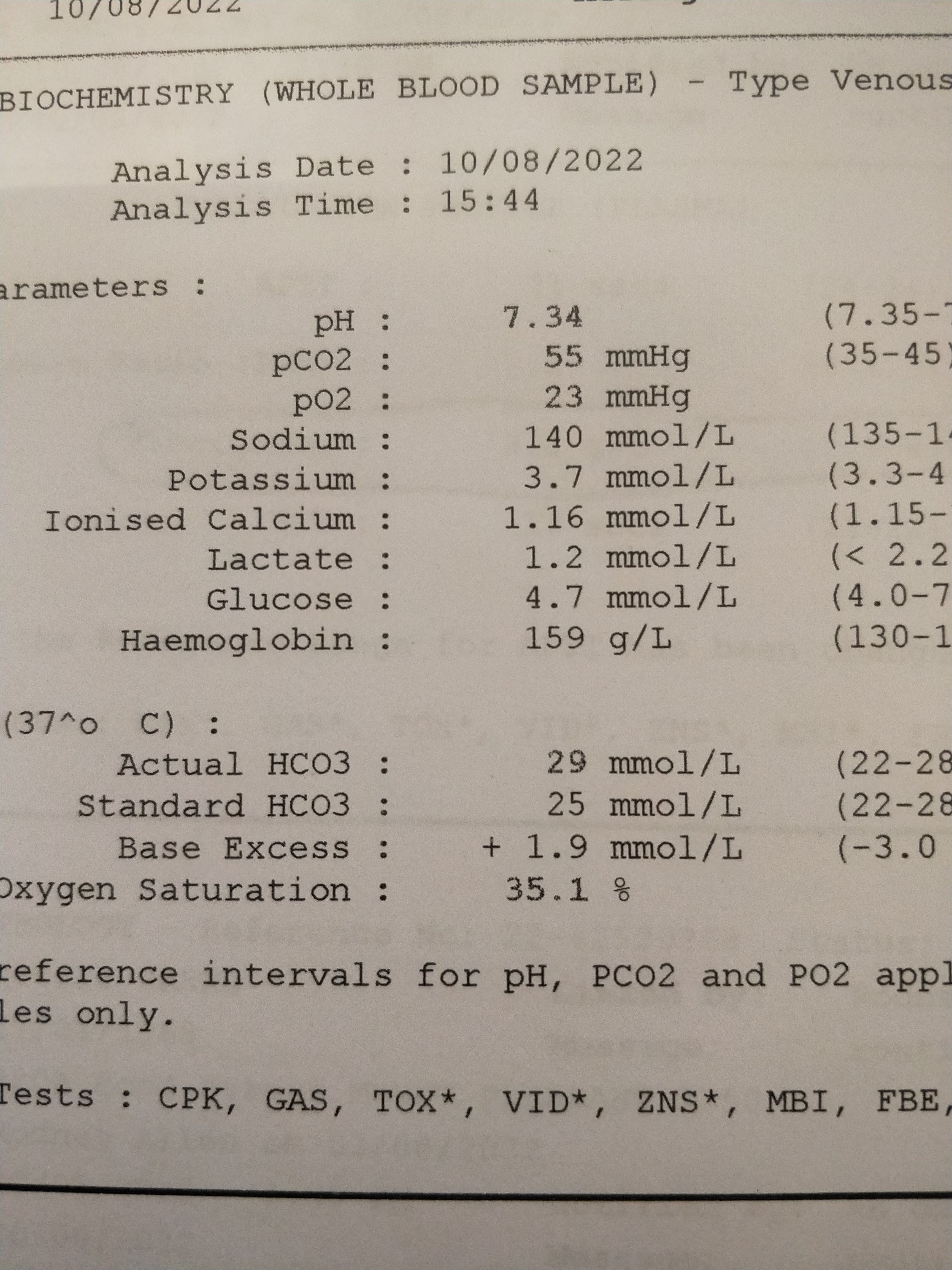
Finally I decided to add Nattokinase and Aspirin to the Vedicinals and after 10 days of combination treatment, I was feeling significantly better and finally, I achieved success! A venous oxygen saturation from 35% to 72%!
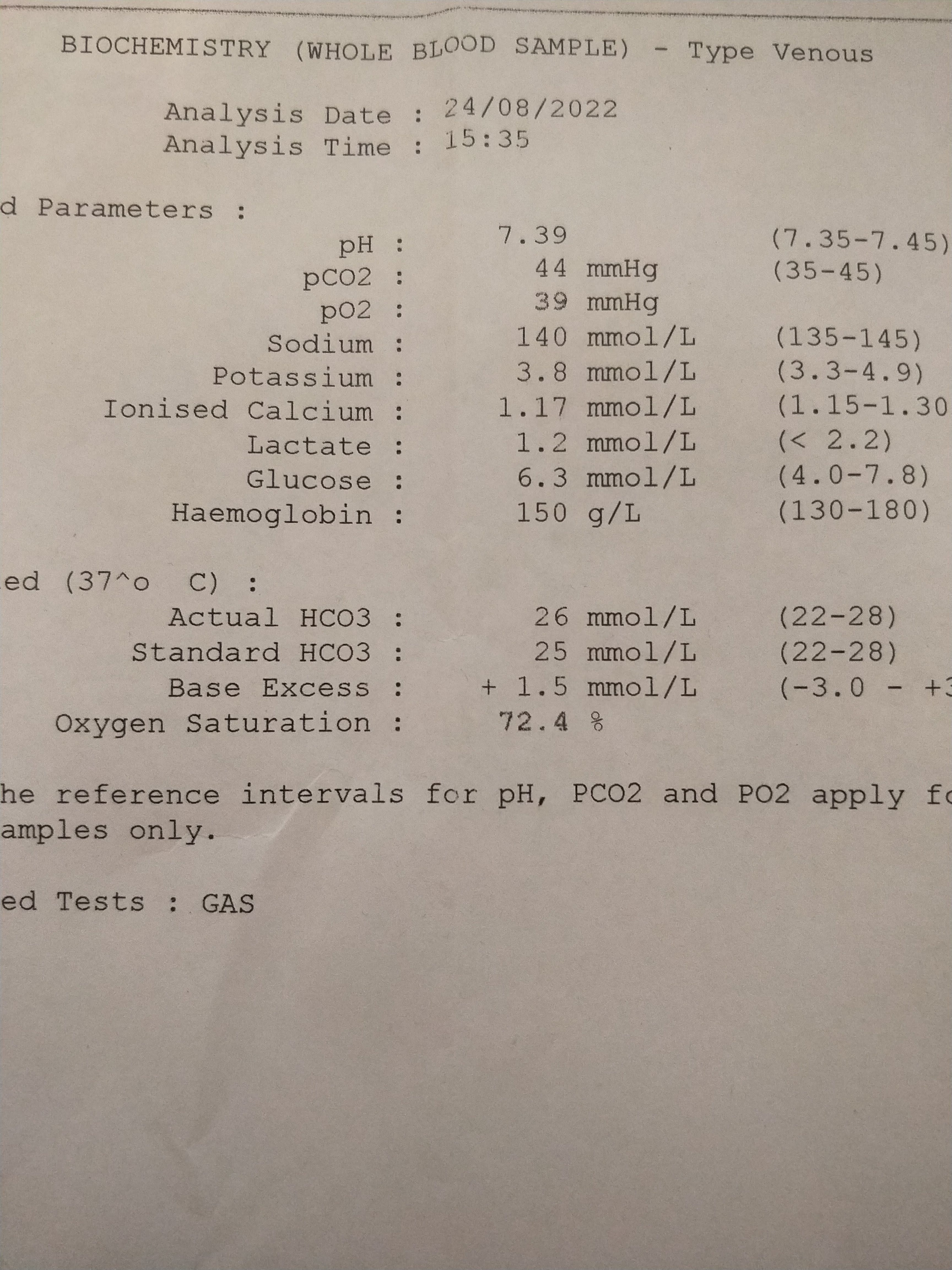
This coincided with me feeling a lot better too. I have continued to feel much better, back to about 80% of my normal capacity, consistently, for months now without significant relapse. I have much less PEM now, and increased ability to focus and concentrate.
What have I learned, and what implications might this have for treatment in general?
It makes sense to start at treating the deepest cause of the disease, then into the more superficial. This is not to say that the more superficial disease processes aren’t just as disabling, it’s just that they are not going to be comprehensively solved until the underlying disease processes that drive them have been dealt with.
In this case, my hypothesis is that even though the manufacturers of Vedicinals claim that it works for every part of long Covid, the reality is that it was specifically designed for acute Covid. For the virus. It’s an antiviral. The only human trial that shows Vedicinals works was in the treatment of acute Covid. Unlike Paxlovid or other antivirals, it is able to be used for chronic Covid, that is, viral persistence, mainly because it is far easier and cheaper to buy privately in the quantities required.
The viral persistence, which likely drives the creation of new microclots, is likely in the gut, so I took probiotics including Lactobacillus Plantarum as well.
I believe that I could not properly clear my microclots until I cleared the viral persistence that kept generating new microclots. Imagine bailing out a leaky boat that keeps filling up, where the “leak” is the viral persistence (probably in the gut) and the “water” is the microclotting. Bailing out the water in the boat is important, but you may not make much progress until you stop the leak.
Why do people get better using just antivirals or just Nattokinase? Or just pacing or Maraviroc or Niacin or antihistamines or fasting or probiotics?
If you think about it, if you only have a small leak or you only have a small amount of water in the boat, bailing the boat out (busting microclots) might work really effectively. This also helps blood flow which helps every other process in the body, including immune function, and the body’s natural virus clearing functions. Imagine little boat patching gremlins that can actually do their job if they’re not drowning. Or perhaps your boat is in a hot climate and the leak isn’t too bad; bailing out the boat might be enough. Or just fixing the underlying infection might be enough; seal the boat and you might not even have to bail out the water because it will just evaporate in the sun.
This speaks to the differences of people with long Covid, that is, we all probably have varying levels of different components of long Covid going on in us. Some of us will get better with one treatment, others will need the whole kit and kaboodle.
But it makes sense to start at the base and work up. Start with the deepest cause. This may not be infection either; if you are vaccine injured then by definition it cannot be. In this case, perhaps it’s immune dysfunction, perhaps abnormal immune cells harbouring spike protein. In this case perhaps something like Maraviroc is what’s needed. Maraviroc deserves a whole post on itself, which I will do in future. Make sure you subscribe!
But perhaps some of these treatments didn’t work for you because these act at places downstream from the main problem; and perhaps these other treatments WILL work once the underlying problem is dealt with.
Postscript:
I remain on the triple combination of Vedicinals, Nattokinase and Aspirin. Whenever I go off of any one of these I start to relapse. I believe that the Vedicinals is keeping my chronic Covid infection in my intestines suppressed, but cannot yet eliminate it. I look forward to further experiments especially with other antivirals to see if I can eliminate the viral persistence for good. I don’t think the infectious leak in my boat body is fully sealed, and until it is, I’m going to have to keep bailing out the microclots from my circulatory boat.
If you’re interested in joining a dynamic group of Long Covid pioneers, performing self experiments and reporting the results using as much objective information as possible, you’re invited to join this Facebook group I started. There are thousands of clever and kind people recovering there!
https://www.facebook.com/groups/829213261296558/
You’re invited to follow me on Twitter too where I stress test my ideas with the Long Covid Brains Trust!
https://twitter.com/AtelierDanko
Really cool approach to detecting microclots, and so glad you found a way to start feeling better. Awesome to see the biomarker both responds to treatment and correlates well with how you're feeling, too.
I'd be curious what the level of agreement is vs. pulse oxygenation. As you said it's (usually?) arterial so probably misses the downstream step of blood --> tissue perfusion.
I wonder if expired gas analysis, like they do in vo2 max tests, could be another proxy. If, at rest, your body is consuming less oxygen, maybe that indicates issues with tissue o2 uptake.
Just requested to join your facebook group!
I've tried about 20 different meds and supplements over the last 6 months and the only two I can swear by is Aspirin and NK. It's nice to read, retrospectively a bit of validation from someone more educated than me on the topic.
I've recently started NAC, CBD Oil (no THC), Ubiquinol and taking Ivabradine to calm the POTS symptoms.
I'll also be starting LDN with the hope that it just eases some of the obvious inflammatory effects while we wait for more detail on how to treat the root cause.
Best wishes